
When reading Action Statement 1 of the 2026 DCD Clinical Practice Guideline, I think of the PT's role as helping the team organize four folders.
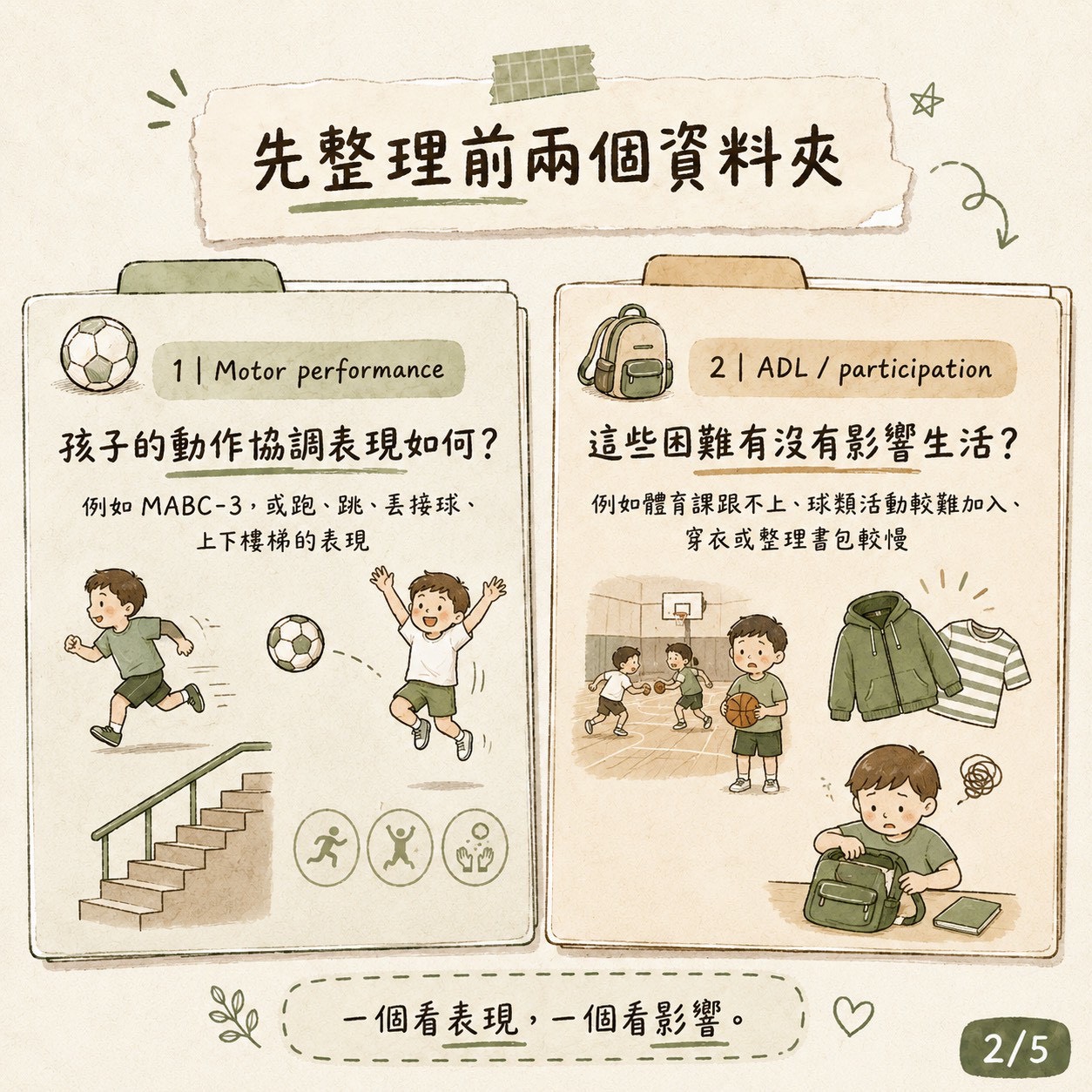
Folder 1: Motor Performance
How is the child's motor coordination performance? For example, MABC-3 results, or the performance in running, jumping, throwing and catching, and going up and down stairs observed during the assessment.
Folder 2: ADL / Participation
Do these motor difficulties affect daily life? Such as falling behind in PE class, finding it hard to join ball games, or being slower in dressing or packing a backpack.
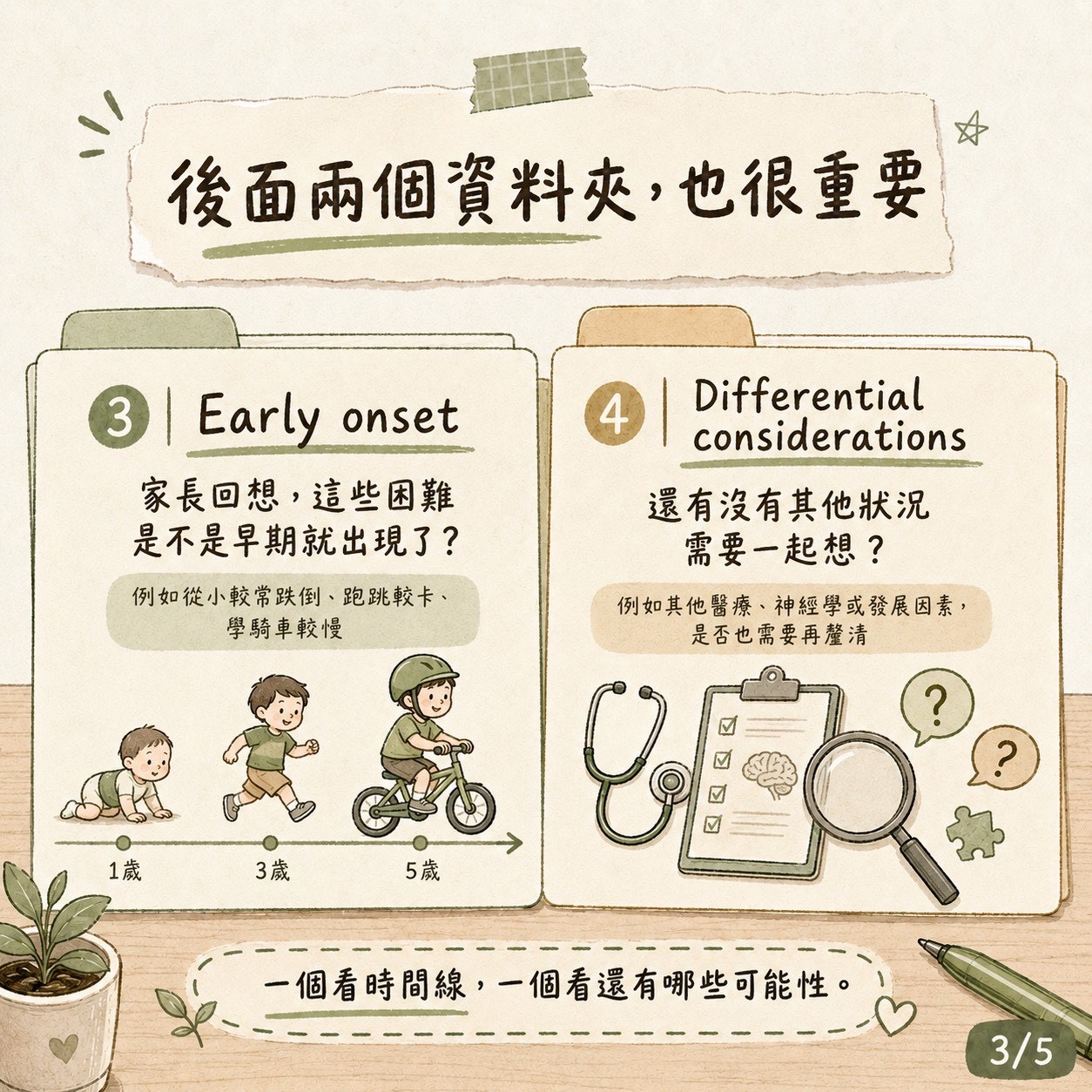
Folder 3: Early Onset
Looking back, parents may recall if the child has fallen more frequently since childhood, seemed clumsy when running or jumping, or struggled more with learning to ride a bike or participate in ball games.
Folder 4: Differential Considerations
Could these performances be related to other medical, neurological, or developmental conditions? Is there anything that needs to be clarified further with the physician or the team?
The Role of PT in Assessment
PTs do not directly diagnose DCD, but the motor observations, daily life contexts, developmental history, and clinical judgments we provide are often crucial puzzle pieces for the team to understand the child.
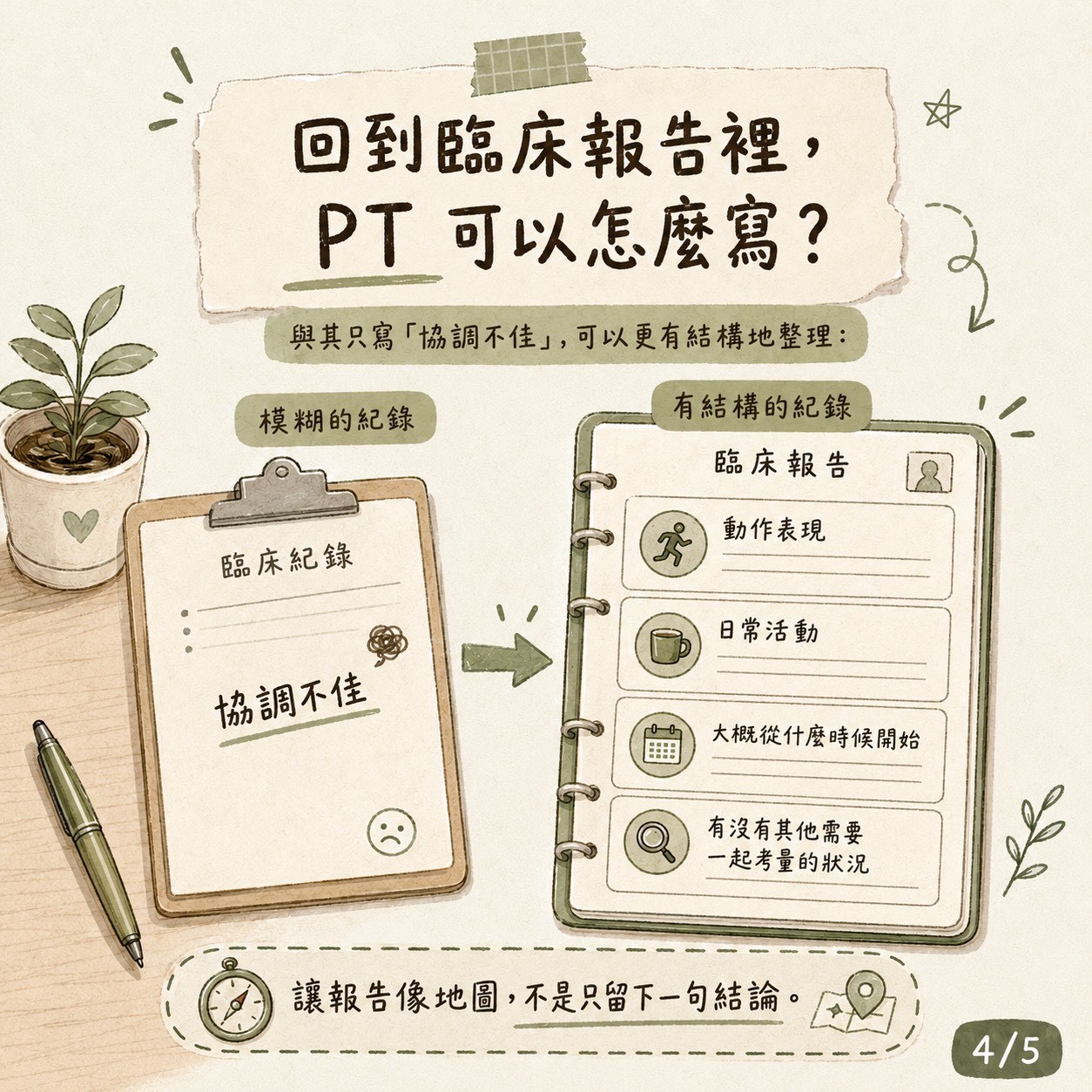
Returning to the report, perhaps we can use less vague terms like "poor coordination" and provide more specific descriptions: in which activities the child struggles, for how long, and what impact it has on their life.
This kind of assessment data is more like a map. When the team, parents, and teachers read it, they will have a better idea of what the next steps can be.
➜ Want to schedule a motor coordination assessment for your child? Welcome to contact us via LINE
References
- Sargent, B., Mueller, M., Iverson, E., Frazier, M., & Kaplan, S. L. (2026). Physical therapy management of children with developmental coordination disorder: A 2026 evidence-based clinical practice guideline from the American Physical Therapy Association Academy of Pediatric Physical Therapy. Pediatric Physical Therapy, 38, 297–333.